

IG023: Guideline on Rodent Surgery and Medical Records
IACUC Guideline Number: IG023, Approved By: IACUC, Approval Date: 8/14/2025, Version: 9
Pupose:
These guidelines provide information for personnel planning surgical procedures and anesthesia/analgesia regimens for rodent species at Michigan State University (MSU). Research animals used for biomedical and training purposes are required to follow the criteria set forth in The Guide for the Care and Use of Laboratory Animals (IRC, 2011). All personnel performing surgical procedures must be appropriately trained and listed on an approved IACUC protocol. Any deviations from these guidelines are to be included and scientifically justified in the protocol. Veterinary questions should be directed to Campus Animal Resources (CAR) veterinary staff (carvets@msu.edu). Surgical and anesthesia training can be scheduled upon request by emailing cartrain@msu.edu.
Guideline:
1: Surgical Principles
For most rodent surgery needs, a facility may be compact and basic, such as a dedicated space within a research laboratory that is appropriately managed to minimize contamination from other ongoing activities in the laboratory. In general, a rodent surgery area should have the following components:
- A place for cages of rodents awaiting surgery.
- An animal preparation area, away from the surgery area, for hair removal and initial skin preparation.
- A surgery space that is uncluttered and easily sanitized.
- A holding and quiet recovery area where the animals can be continuously observed until fully recovered from anesthesia.
- Limited access permitted to only those personnel involved in performing or assisting with the procedure.
A. Non-Survival (Terminal) Rodent Surgery
Aseptic technique recommended but not required: For surgical procedures from which animals will not recover from anesthesia (non-survival or terminal surgery), surgeons must be qualified and trained to ensure that adequate depth of anesthesia is maintained.
- The surgical area should be clean and uncluttered.
- At a minimum, the surgical site must be clipped, and clean instruments used.
- The surgeon must wear gloves (sterility not required) and appropriate personal protective equipment (PPE).
- Anesthetized animals are not to be left unattended.
- Expired drugs are not to be used. Refer to IG017: Expired Medical Materials.
- Please note: more stringent aseptic practices may be necessary when tissues are manipulated or collected in a sterile manner, or for procedures of prolonged duration during which an infection could occur. These practices must be described in the IACUC protocol.
B. Survival (Recovery) Rodent Surgery
Aseptic technique required: For surgical procedures from which animals will recover from anesthesia (survival or recovery surgery), surgeons must be qualified and trained to ensure that adequate depth of anesthesia is maintained.
The fundamental principle of aseptic surgery is that anything that contacts the surgical site must be sterile. The guidance provided in this document are designed to establish sterility when beginning the procedure and to maintain sterility throughout the procedure.
Instruments
- Instruments, supplies, and devices are to be sterilized (includes: catheters, osmotic pumps, telemetry transmitters, trocars, infusion lines, etc.). See Table 1.
- Segregation of instruments according to function helps maintain aseptic technique (e.g., instruments used on skin should not be used within the abdominal cavity).
- Instruments should be wiped clean of blood and tissues with sterile gauze after use and then sterilized either chemically or mechanically. See Table 1.
- Whole instrument sterilization is to be performed initially using a validated primary sterilization technique (i.e., an autoclaved instrument pack). See Table 1.
- Glass bead sterilizers are not recommended as the primary method for instrument sterilization1. Use of glass bead re-sterilization is appropriate when performed between multiple (batched) surgeries on the same day.
- Multiple rodents (up to 5) can be batched for a survival surgery procedure with re-sterilizing instruments using the glass bead sterilizer between each rodent (5 surgeries per sterilized pack).
- Follow manufacturer recommendations for contact time for instruments in the bead sterilizer. Depending on the size of the instrument, a minimum of 20 seconds contact time is needed.
- Bead sterilized instrument tips must be allowed to cool before use.
- Glass bead sterilizers are not recommended as the primary method for instrument sterilization1. Use of glass bead re-sterilization is appropriate when performed between multiple (batched) surgeries on the same day.
- Bead sterilized instrument tips must be allowed to cool before use.
- Do not use toothed or crushing instruments on rodents to avoid causing unintended tissue damage.
- Close surgical wounds using appropriate techniques and materials. See Table 2.
- Suture material or staples used for skin closure are to be removed after verifying the wound has healed. Sutures/staples are generally removed 7-10 days post-surgery.
| Agents | Examples | Comments |
|---|---|---|
| Steam Sterilization (moist heat) | Autoclave | Effectiveness dependent upon temperature, steam pressure, and time. Verify adequacy of heat through use of temperature tape applied to autoclaved materials to ensure sterilization. |
| Ionizing Radiation | Gamma Radiation | Requires special equipment. |
| Chemical (gas sterilization) | Ethylene Oxide | Requires 30% or greater relative humidity for effectiveness against spores. Requires safe airing time. |
| Suture | Properties |
|---|---|
| Vicryl ® (polyglactin 910) Dexon® (polyglycolic acid) | Braided material; absorbable within 60-90 days. Use to ligate or suture tissues where absorbable suture is needed. |
| PDS® (polydioxanone), Maxon® (polyglyconate) | Monofilament material; absorbable within 6 months. For use in ligation or suturing where extended wound support is needed. |
| Prolene® (polypropylene) | Monofilament material; nonabsorbable. Insert. Used in soft tissue procedures. |
| Ethilon® (nylon) | Monofilament, nonabsorbable. Insert. Good tensile strength and minimal tissue reactivity. |
| Silk | Braided, nonabsorbable. (Caution: can cause tissue reactions and may wick microorganisms into the wound). Used in soft tissue procedures, not for skin closure. |
| Chromic Gut | Monofilament, absorbable within 90-120 days. Soft tissue and ligation procedures; may cause moderate tissue reaction. |
| Stainless Steel Wound Clips, Staples | Nonabsorbable. Requires special instrument for steel/staple insertion and removal. |
| Surgical Adhesive (Vetbond™) | Skin adhesive. Area needs to be dry and free of blood; can cause an exothermic reaction at time of placement on skin so limiting the volume applied is essential. |
Preparation of Surgical Site
- With the animal anesthetized/sedated, position in a location (bench or room) separate from the surgical area.
- Remove hair using electric clippers with an appropriate blade size. Avoid skin abrasions and thermal injuries.
- Depilatory creams (Nair®) may be used to aid in hair removal. Contact time should be limited to no more than 60 seconds and depilatory cream thoroughly cleansed from the area using warm saline to avoid skin irritation.
- Dispose of removed hair to avoid hair from becoming airborne and potentially contaminating the surgical site.
- Do not wet large areas of animal with disinfectant or removal agents as this can exacerbate hypothermia.
- Sterile gauze or Q-tips soaked with skin disinfectant can be used for skin preparations. See Table 3.
- Begin along the incision line with a disinfectant-soaked Q-tip or gauze and extend outward (dirty) towards the center (clean). Discard gauze or Q-tip and use a new one for each sequential scrub.
| Name | Examples | Comments |
|---|---|---|
| Iodophors | Betadine® Prepodyne® Wescodyne® | Inactivate a wide range of microbes but their activity is reduced in the presence of organic matter. |
| Chlorhexidine | Hibiclens® Nolvasan® | Rapidly bactericidal and persistent. Effective against many viruses. Excellent for use on skin. |
| Alcohols | 70% ethyl alcohol 70-99% isopropyl alcohol | Not deemed adequate for use alone. Not a disinfectant/sterilant. Only for use to remove excess scrub. Follow MSU Environmental Health and Safety (EHS) guidance for use of isopropyl alcohol (https://ehs.msu.edu/lab-clinic/chem/peroxide-formers.html). |
| Waterless alcohol-based antiseptic | Avagard™ | Effective surgical skin preparation with 1 or 2 applications only. Mitigates intraoperative body temperature loss compared to aqueous agents. |
Chlorhexidine and waterless alcohol-based scrubs can be used without an alternate scrub. Iodophor scrub should be alternated 3 times with alcohol/room temperature sterile saline, followed by a final prep with an iodophor solution. Scrub surgical site up to 3 times and leave on skin for at least 2 minutes prior to creating the incision. Remove excess liquid with dry sterile gauze.
Surgeon Scrub Preparation:
The purpose of the surgeon’s scrub is to remove dirt and decrease the bacterial flora on the surgeon’s hands and arms prior to donning surgical gloves and initiating surgery. Certain agents used during the surgical prep of the surgeon contain residual antibacterial activity which helps decrease bacterial levels under surgical gloves. Depending on the availability of surgical assistants, the solo surgeon often will need to open a sterile instrument and drape pack and sterile glove pack before commencing the scrub preparation.
- Put on surgical mask and clean lab coat or disposable PPE gown. Surgical cap is recommended.
- Thoroughly wash hands with a sanitizing soap.
- Put on sterile gloves; gloves may be surgical style (individually packaged – recommended) or autoclaves nitrile laboratory gloves.
- Do not touch any non-sterile surfaces. If the gloves touch non-sterile surfaces, gloves should be replaced with a new sterilized pair.
Draping:
- Drape the surgical site such that the skin targeted for incision is accessible, but the animal is not entirely covered.
- The use of transparent draping material (e.g., Glad Press’n Seal; 3M Tegaderm) over the surgical site provides an appropriate view of animal respirations and any potential complications that a full towel or opaque drape will not.
- Do not completely enclose the rodent in the transparent drape to prevent overheating of the animal.
Maintaining Sterility:
- The surgeon should restrict their contact to the surgical site, using only sterilized equipment until the incision is closed.
- ALWAYS put sterile equipment on a sterile surface (sterile surgical tray, sterile towel or drape, or sterile gauze) when not in use.
- The surgeon should not touch anything that is not sterile once gloves are put on.
- The tips of sterilized instruments should be used to manipulate and handle tissues.
- Minimize exteriorizing organs, but, if necessary, please tissues on sterile gauze adjacent to incision and keep moist with sterile saline until replacement into the abdominal cavity.
- If instruments are being used on multiple animals, a hot-bead sterilizer may be used to sterilize the instrument tips.
2: Anesthesia and Analgesia
A. Anesthesia
- It is not necessary to withhold food from rodents for more than 4 hours to fast them before surgery. Their short gastrointestinal tract and high metabolic rate will eliminate food from the stomach rapidly. Rodents are also unable to vomit so risk of aspiration is minimized.
- Analgesia should be given preoperatively; see analgesia section below.
- Following induction of anesthesia, apply a sterile ophthalmic lubricant (e.g., Puralube® Vet Ointment), to the eyes (~0.5 cm strip per eye) to prevent ocular irritation and corneal drying.
- The animal must be maintained at a surgical plane of anesthesia throughout the procedure. Vital signs of the animal are to be monitored throughout the procedure (such as: respiratory rate, skin color, non-responsive to toe pinch).
- Anesthetic technique should be delivered as described in the specific approved IACUC protocol.
- It is recommended that 100% oxygen be supplied to all rodents anesthetized with injectable drugs. Small animals, particularly mice, breathing room air following administration of injectable anesthetic drugs become hypoxic (i.e., decreased oxygen levels in the blood). Hypoxia may lead to complications including delayed anesthetic recovery or death.
- If delivering gas anesthesia, appropriate waste gas scavenging must be used to avoid personnel exposure.
Note: Contact Environmental Health & Safety (EHS) at ehs@msu.edu for assistance with gas scavenging systems.
| Anesthesia | Species | Dosage (mg/kg) (unless specified) | Duration of Anesthesia | Route of Administration |
|---|---|---|---|---|
| Ketamine (CS) (K) / Xylazine (X) | Mice | 80-120 (K) / 5-10 (X) | 30-45 min | IP |
| Ketamine (CS) (K) / Xylazine (X) | Rats | 40-90 (K) / 5-10 (X) | 45-90 min | IP |
| Ketamine (CS) (K) / Xylazine (X) / Acepromazine (A) | Mice | 80-100 (K) / 5-10 (X) | 40 min | IP |
| Ketamine (CS) (K) / Xylazine (X) / Acepromazine (A) | Rats | 50 (K) / 5 (X) / 1 (A) | 30-45 min | IP |
| Ketamine (CS) / Dexmedetomidine (D) | Mice | 50-75 (K) / 0.5-5 (D) | 20-30 min | IP |
| Ketamine (CS) / Dexmedetomidine (D) | Rats | 75 (K) / 0.25-0.5 (D) | 120 min | IP |
| Isoflurane | All Rodents | 1-5% (to effect) | As long as agent is provided | Inhalation |
(CS) = Controlled Substance. Special licensing through the Drug Enforcement Agency (DEA) is required to procure and prescribe these agents. Contact ehs@msu.edu for more information regarding DEA licensing.
B. Analgesia
A foundational assumption of the US Government Principles (1985) is that if a procedure would be likely to cause pain or distress in a human, then it is likely to do so in animals; therefore, measures should be taken to ensure welfare of animals in research. Adherence to federal policies and regulations, as well as to the 3R’s (Reduction, Replacement, and Refinement) of animal research necessitate the use of drugs to alleviate pain and distress associated with research procedures. The IACUC has determined that analgesia must be provided in all such cases unless non-administration has been scientifically justified in the animal protocol and approved by the IACUC.
Analgesia is most effective if it is administered prior to commencement of the surgery (preoperative or preemptive), followed by additional analgesics given postoperatively. Multimodal therapy (e.g., use of a local skin anesthetic and a NSAID or opioid) provides broader coverage of pain receptors and is recommended. The level, type, and duration of analgesia will depend upon the procedure performed. For postoperative analgesia, minimally invasive procedures need less potent or shorter-acting analgesics and may respond to a single dose of analgesic. More invasive procedures (e.g., laparotomy, orthopedic surgery) may require multiple doses of analgesic for up to 72 hours postoperatively. Specific criteria for evaluating pain and provision of analgesia are to be developed through veterinary consult and described in the IACUC protocol. It is the responsibility of the investigator and staff to evaluate the animal on a routine basis and determine, in consultation with CAR veterinarians, whether additional treatment is warranted based upon protocol criteria.
| Anesthesia | Species | Dosage (mg/kg) (unless specified) | Frequency of Administration | Route of Administration |
|---|---|---|---|---|
| Buprenorphine HCI (CS) | Mice | 0.1 - 0.5 | 4 – 6 hrs. | SC |
| Buprenorphine HCI (CS) | Rats | 0.05 – 0.1 | 6 – 8 hrs. | SC |
| Buprenorphine SR and Ethiqa XR2 (CS) (sustained release) | Mice | 0.5 – 11 3.252 |
48 – 72 hrs. | SC |
| Buprenorphine SR and Ethiqa XR2 (CS) (sustained release) | Rats | 1.21 0.652 | 48 – 72 hrs. | SC |
| Butorphanol (CS) | Mice | 5 | 1 – 2 hrs. | SC |
| Butorphanol (CS) | Rats | 1-2 | 1 – 2 hrs. | SC |
| Carprofen (Rimadyl®) | Mice | 5 | 12 – 24 hrs. | SC |
| Carprofen (Rimadyl®) | Rats | 5 | 24 hrs. | SC |
| Ketoprofen | Mice | 5 – 20 | 24 hrs. | SC |
| Ketoprofen | Rats | 5 | 24 hrs. | SC |
| Meloxicam | Mice | 5 – 10 | 8 – 12 hrs. | SC, PO (oral suspension) |
| Meloxicam | Rats | 1 | 12 – 24 hrs. | SC |
| Morphine (CS) | Mice Rats | 10 | 2 – 3 hrs. | SC |
| Tramadol (CS) | Mice | 80 | 24 hrs. | SC |
| Tramadol (CS) | Rats | 5 | 24 hrs. | SC |
(CS) = Controlled Substance. Special licensing through the Drug Enforcement Agency (DEA) is required to procure and prescribe these agents. Contact ehs@msu.edu for more information regarding DEA licensing.
C. Local and Topical Anesthetics
Local anesthetics can reduce the perception of pain at the surgical site; these should be infiltrated around the incision site prior to recovery of the animal from general anesthesia, and preferably prior to the incision being initiated. In conjunction with other agents, their use may allow reduced levels of general anesthetics, which may speed recovery and minimize potential for adverse outcomes.
| Local or Topical Anesthetics | Species | Dosage (mg/kg) (unless specified) | Route of Administration |
|---|---|---|---|
| Bupivacaine | Rodents | 0.25-0.5%, not to exceed 5 mg/kg | Local infiltration; SC around incision site |
| EMLA® May take 30 min for effect | Rodents | Application of a layer up to 1mm thickness | Topical application |
| Lidocaine (2%) | Rodents | Dilute to 0.5%, not to exceed 4 mg/kg | Local infiltration; SC around incision site |
| Proparacaine (0.5%) | Rodents | 1-2 drops per eye | Topical applied to eye prior to staining the cornea or prior to RO sampling |
D. Reversal Agents
Reversal of certain drugs leads to early termination of anesthesia, which may reduce adverse events and allow rapid return of the rodents to the home cage environment. If reversal agents are used, both the anesthetic and analgesic properties of the drug may be terminated, thus alternative sources of analgesia should be provided.
| Reversal Agents | Used to Reverse | Species | Dosage (mg/kg) (unless specified) | Route of Administration |
|---|---|---|---|---|
| Yohimbine | Xylazine | Mice | 1 - 2 | SC |
| Atipamezole (Antisedan®) | Dexmedetomidine (Dexdomitor®), Xylazine | Rodents | 0.5 – 1.0 | SC |
| Naloxone | Opioids | Rodents | 20 | IP |
3: Monitoring of the Animal
A. Confirmation of Anesthesia Depth
The animal is to be maintained at an appropriate depth of anesthesia beginning immediately before the surgical procedure is initiated, through the conclusion of the procedure, and until the postoperative analgesics have taken effect. For most species, the following techniques can be used to ascertain that the animal is appropriately anesthetized.
- Toe pinch: brief clamping of the web of skin between toes or claws with a hemostat or fingers. Firmly pinching multiple toes should not elicit a withdrawal response from an animal at a surgical depth of anesthesia.
- Palpebral reflex: gently tapping the medial canthus of the animal’s eye should not elicit a blink or eye flutter. This technique is not always reliable in all animals.
- Corneal reflex: touching the edge of the cornea with a gauze sponge or cotton swab will produce a good reflex if the patient is too light on anesthesia. Movement of the eyelids is an indication that the depth of anesthesia is not sufficient to do surgery.
- Vital signs: heart rate and respiratory rate may increase if anesthetic levels become too light.
B. Maintenance of Anesthesia
- Each animal responds differently when under anesthesia, therefore it may be necessary to modify your use of anesthetics during the procedure. All routinely used anesthesia options are to be described in the IACUC protocol. Personnel need to be trained in not only delivering the anesthetic to the patient, but also in identifying anesthetic related problems.
- Increases and decreases in vital signs (see Monitoring Vital Signs below) may require modifications in anesthetic dosing.
- If, at any time, an animal begins to respond to pain or attain an anesthetic depth that is too light, stop the procedure and adjust the inhalant anesthetic level or give a supplemental dose of injectable anesthetics. Reassess the animal before resuming work.
- Animals need to be continually monitored while anesthetized and receive appropriate anesthesia and life support for the duration of the procedure. Anesthetized animals are NOT to be left alone during the procedure.
- To maintain sterility during complex surgical procedures and to properly monitor the animals, it may be necessary to include a second person in the procedure for assistance.
C. Monitoring Vital Signs During Surgery
Personnel should continuously monitor the animal’s basic physiological function for the duration of the procedure – from induction of anesthesia through recovery. At a minimum, the following vital signs are to be monitored during all procedures involving rodents. CAR veterinary staff are always available to assist in choosing an appropriate method for monitoring the rodent species involved.
- Respirator rate can be assessed by watching the rising and falling of the chest cavity. Any changes in respiration should be addressed by altering the depth of anesthesia.
- Body temperature should be maintained near normal during surgical procedures.
- Depth of anesthesia should be assessed by periodic checking of response to tactile stimuli (toe pinch, corneal reflex, etc.).
D. Heat Loss
Maintenance of normothermia (a clinically appropriate body temperature) is critical for welfare and facilitates recovery of rodents from anesthesia. Warm water recirculating blankets at 370C, warmed (body temperature) fluid bags, or thermal discs are to be used, or the animal will become hypothermic during the course of surgery. Rodents are extremely susceptible to hypothermia which often occurs due to anesthesia-induced vasodilation and from heat loss via opened body cavities.
- When using warming devices, they should be covered such that no animal is placed directly on a warmed surface.
- Monitor microwaveable discs to ensure they are not TOO HOT before exposing an animal to them.
- Heat lamps need to be used with caution to avoid overheating rodents.
- Heat should be provided during surgery and throughout the recovery period.
- No matter the type of heat source provided, ensure that the animals have a non-heated part of the recovery cage which they can access to avoid overheating or hyperthermia.
IMPORTANT: Due to the inconsistency of heating and history of thermal burns in small animals, electric heating pads are not to be used for rodent species.
E. Fluid Loss
Fluid loss occurs because of evaporation from body cavities and blood loss; during surgery with anesthesia, all animals (including humans) lose fluids. Rodents are vulnerable to the effects of fluid loss because of their small size and high metabolic rate.
- Offset the potential for surgical fluid loss by:
- Irrigating the operative field with warm sterile saline.
- Controlling blood loss.
- Administering warm sterile fluids (up to 1ml for mice and 3ml for rats intraperitoneally or subcutaneously) pre-procedurally, with additional fluids provided post procedure if notable fluid loss occurred.
4: Postoperative Care
Animals need to be monitored continuously during the surgical procedure and then every 10-15 minutes until fully ambulatory. These checks should be documented.
- Body temperature should be maintained.
- Place animal in a clean, dry cage and provide warmth. Ensure that the animal has a non-heated part of the recovery cage which they can access to avoid hyperthermia.
- House rodents individually until they are ambulatory to prevent injury or suffocation. Do not return them to animal housing until they are conscious and mobile.
- Post-surgical animals should be observed daily for a minimum of 3 days (72 hours) after the procedure by a member of the PI’s staff or other identified trained individual to ensure that there are no complications. This includes holidays and weekends. Observations should include:
- Monitor for signs of pain and distress (see below).
- Assess the animal’s behavior, respiration rate, and activity.
- Assess appearance and condition of the surgical site.
- For at least 3 days (72 hours) following the procedure, daily observations of the animal’s condition must be recorded in the medical record. These entries should include details of the animal’s clinical status and documentation of analgesic administration, including drug names, dosages, and times given.
- Administration of analgesics and postoperative monitoring of animals is to be consistent with the description provided in the approved protocol.
- If the PI or staff finds that an animal appears ill, or the surgical wound appears abnormal, contact the CAR veterinary staff immediately.
- DietGel may be provided to rodents during the postoperative period as an extra source of nutrition to aid in recovery. If a lab chooses to provide DietGel, it is recommended that DietGel be provided 1-2 days prior to surgery so animals may acclimate to the alternate food source. A ½ cup of DietGel can be provided per day in addition to the standard rodent chow. DietGel should be replaced daily or when visibly dried out or soiled. Potential signs associated with pain or distress in rodents:
- Decreased food and water consumption, weight loss
- Self-imposed isolation/hiding
- Rapid, open mouth breathing
- Biting, aggression
- Increased/decreased movement, twitching, trembling
- Unkempt appearance (rough, dull hair coat)
- Abnormal posture/positioning (hunched back, head-pressing)
- Dehydration, skin tenting, sunken eyes
A. Suture / Staple Removal
Sutures or staples are to be removed 7-10 days post-procedure (unless exempted in the protocol), and the date of removal recorded in the record. The surgical records will be maintained for as long as the animal is housed in MSU facilities. After termination of the animal, the surgical records for non-USDA covered species will be maintained as the PI deems appropriate. The PI will maintain records for USDA covered species for 3 years after the animals’ termination.
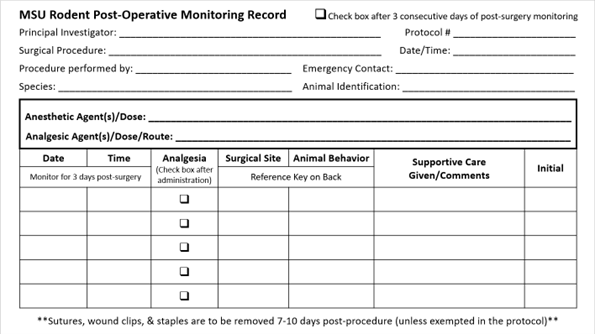
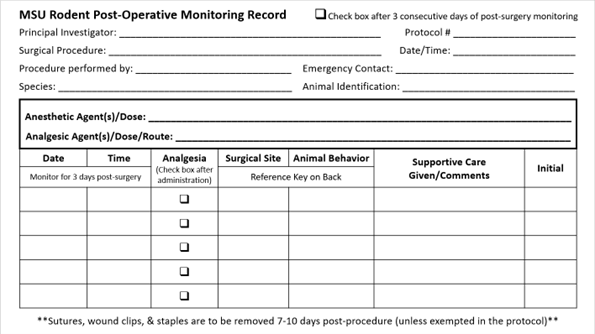
B. Surgical/Medical Records
Records should include the following information:
- Animal identification
- Surgical procedure and date procedure was performed
- Principal Investigator and name of the person doing the procedure
- Anesthetic agent(s) used and dose
- Analgesic agent(s) used and dose
- Observations during and after surgery
- Date sutures removed, if applicable
- Emergency contact information
- Postoperative notes
The MSU IACUC expects that perioperative records will be maintained on all vertebrate animals undergoing survival surgery.
Postoperative observations and treatments are to be recorded and initiated on each date performed. The weight of the animal should also be recorded in the daily log, if indicated in the IACUC protocol. If the protocol states that food and water consumption will be monitored postoperatively, these observations should be recorded in the daily log. All daily entries should be legible.
Potential operations for maintaining perioperative records:
- The records may be kept on 3”x5” cards maintained behind the cage card in the cage cardholder. Card may be removed from cage when observations are no longer needed. Please save for your records.
- Records may be maintained in a notebook which is kept in the animal room or in the laboratory. Cages must be labeled with a date and procedure performed. Record may be removed from room when observations are no longer needed. Please save for your records.
- In general, regulatory agencies require medical records and records of disposition be kept for 1 year. However, some funding agencies and publishers may require a longer period of record retention. Check with your agencies and editors for their requirements.
If option 1 or 2 is not possible, other arrangements should be described in the protocol and approved by the IACUC.
Sample of 3” x 5” card. [Cards can be obtained from CAR] – FRONT
Sample of 3” x 5” card – BACK
References:
- 1Skiles B, Johnston NA, Hendrix GK, Hickman DL. Effectiveness of the Glass Bead Sterilizer for Sterilizing Surgical Instruments. J Am Assoc Lab Anim Sci. 2022 May 1;61(3):252-255
- Guide for the Care and Use of Laboratory Animals, 8th Edition, National Research Council, 2011.